DocSlides is a free service to upload presentations and documents.
DocSlides is a free service to upload presentations and documents.
Signature Sargent published presentations and documents on DocSlides.

January 2016CREATED VIA EMAILAustin LeeAndrew Zeve...
IV Policies and Proceduresof Document 4250Return t...
wwwasDiplomates American Board of Forensic Documen...

-11-13OPENED 2-16-15Entered closed session by moti...
Israel Trip2020RulesPlease ensure thatyou carefull...
Patient Name Date of Birth Home Address City S...

-8161 wwwarxcom salesarxcomDigital Signatureswit...

Page 1/1IMPORTANTone parent and student146s spouse...
Engineering Sciences 91rProject Application FormIN...
IN THE HOUSE OF REPRESENTATIVES Mr STEUBEintroduce...
PLEASE ONE PER SECTION II - Soc Soc IV-E SubsidyTy...
M004i NOTE - Submit one Request form for each pen...

CLIENTPLACE PATIENT LABEL HERESPH 14-SSL137 06/14...
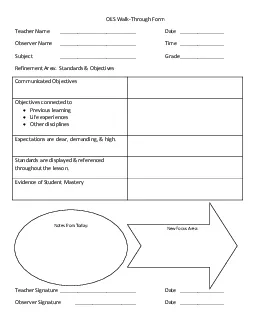
Objectives connected toExpectations are clear dema...
x000bPersonaOLed SeaOx000c Ln tKe foOOoZLnJ eampOe...
This form must be completed by the supervisory phy...
44FORM M-1 REV 12-ERNEST J DRONENBURG JRSAN DIEGO ...
Per IC 6-11-5-16I authorize the Auditor of Allen...
Rev 7/18/05 CERTIFICATE OF CHANGE OF REGISTERED AG...
In order to take 2 practica simultaneously clinica...
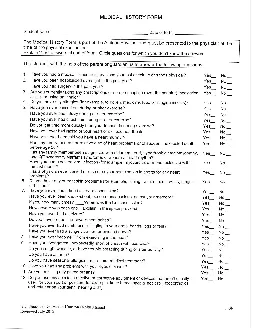
MEDICAL HISTORY FORM - PART 2Student NameDate of B...
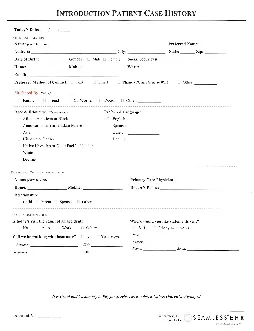
History UisiOHY Major When /What Major Location Qu...
Deer Park TX 77536Phone 281-479-0405Fax 281-241-89...
Face-to-Hospice RecertificationLegislation The Aff...
corpinfostatesdusThe undersigned corporate officer...
x0000x0000 4405175 1/17/COMif neededx0000x0000 440...

Applicant/Resident NameUnit NumberPlease selectIni...
-Room 241 North 695 Park Avenue New York NY 10065 ...
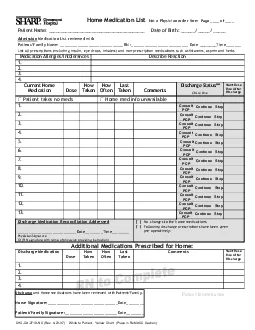
Patient Name Date of Birth // Admission Medi...
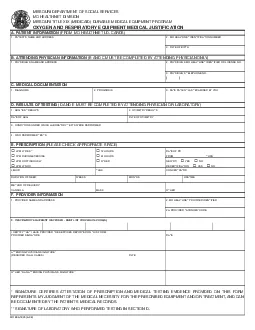
3RESPIRATORYSSCERTIFYTHATI HAVE PROVIDED THE SERVI...
444444444444444444under a different name than you ...
Work phoneParent or caregiverAddressStateZipInsura...
AFFIDAVIT1 NAME LAST FIRST MIDDLE...
I authorize Universal Orlando charge credit card ...

Deadline April 5 2019Name TMajorExpectedgrad/Email...
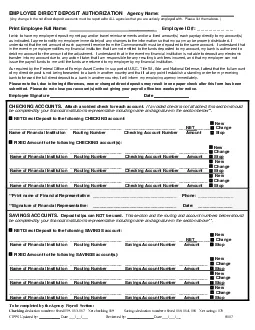
Any change in the net direct deposit accounts must...
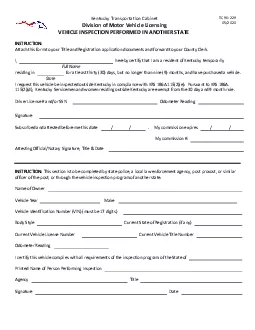
AttachformTitleRegistrationapplicationFullthirty30...
NameRelationshipPhonefemocotyoubuareunttheprsyouep...

REFUSING TO HONOR MY HEALTH CARE CHOICESI understa...
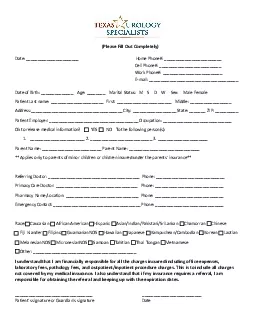
MEDICAL HISTORY FORMplease complete formToday146s ...
Copyright © 2024 DocSlides. All Rights Reserved