DocSlides is a free service to upload presentations and documents.
DocSlides is a free service to upload presentations and documents.
Key Signature published presentations and documents on DocSlides.
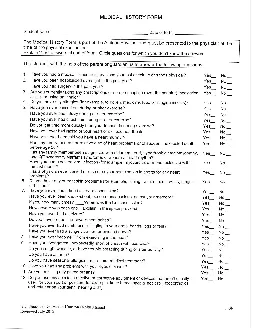
MEDICAL HISTORY FORM - PART 2Student NameDate of B...
History UisiOHY Major When /What Major Location Qu...
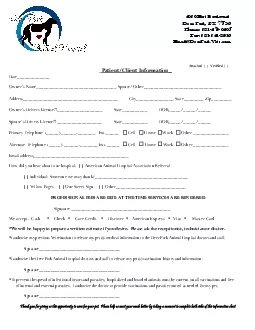
Deer Park TX 77536Phone 281-479-0405Fax 281-241-89...
Face-to-Hospice RecertificationLegislation The Aff...
corpinfostatesdusThe undersigned corporate officer...
x0000x0000 4405175 1/17/COMif neededx0000x0000 440...

Applicant/Resident NameUnit NumberPlease selectIni...
-Room 241 North 695 Park Avenue New York NY 10065 ...
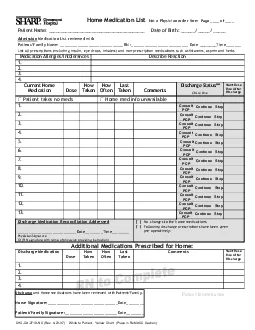
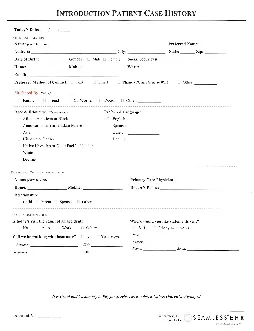
Patient Name Date of Birth // Admission Medi...
3RESPIRATORYSSCERTIFYTHATI HAVE PROVIDED THE SERVI...
444444444444444444under a different name than you ...
Work phoneParent or caregiverAddressStateZipInsura...
AFFIDAVIT1 NAME LAST FIRST MIDDLE...
I authorize Universal Orlando charge credit card ...

Deadline April 5 2019Name TMajorExpectedgrad/Email...
Any change in the net direct deposit accounts must...
AttachformTitleRegistrationapplicationFullthirty30...
NameRelationshipPhonefemocotyoubuareunttheprsyouep...

REFUSING TO HONOR MY HEALTH CARE CHOICESI understa...
MEDICAL HISTORY FORMplease complete formToday146s ...
Account NumberTodayx0027s DateJoint Owner Name inc...
tuition fees Student must initial by hand to appro...

l107 W 16thStStorm Lake IA 50588 712 732-2033NE...
Eligible to pitchagain on date DatePitchesPitchers...
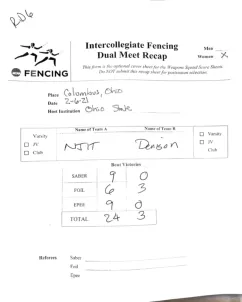
-----------D FENCING DUAL MEET SCORESHEET O Men Wo...
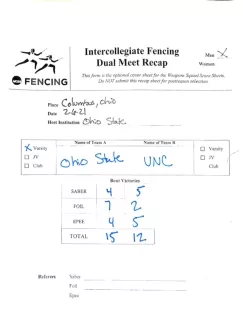
b Do NOT sA Name of T I I Referees Signature -----...
x0000x0000REV 11/6/2018PLEASE PROVIDE A COPY OF TH...
Applications for AdmissionIf you are not registere...
IN THE HOUSE OF REPRESENTATIVES Mr STEUBEintroduce...
SAMPLEName Enterederm aneENGNURSBSN ncentratio...
Retain this form for your records It is your proof...

NameIDDe AnzaCollegeFinancialAidRequestfor reviewD...

Check only if the type applies to the Limited Liab...

TRICARE NONNETWORK CERTIFIED REGISTERED NURSE ANES...
FwwworegonvotesgovCounty Cityand District Candidat...

General STATEMENT OF INTENT TO EMPLOY CDE Form B1-...

ITD 3522 Rev 09-21Supply This certification is u...
STEVENBOX1599107DMVDRIVEKILMARNOCK2248280443531038...
-19 VACCINE FORMLast NameFirst NameDOB Primary Car...
ientirstSecuridrestretatHCelltaSinarratePriDateAge...
Copyright © 2024 DocSlides. All Rights Reserved