Explore
Featured
Recent
Articles
Topics
Login
Upload
Featured
Recent
Articles
Topics
Login
Upload
Search Results for 'insurance address'
insurance address published presentations and documents on DocSlides.
MOBILE INSURANCE WORKSHOP
by avantspac
MOBILE INSURANCE AND REGULATORY FRAMEWORKS. Fangma...
Texas Department of Insurance www
by conchita-marotz
tdi texas gov FIN535 0 115 PUBLIC INSURANCE ADJ U...
BEFORE THE COMMISSIONER OF INSURANCE
by jaena
OF THE STATE OF KANSASIn the Matter of the Kansas ...
John P Tanner DDS MD
by ella
FACIAL SURGERY GROUP Patient Information Kasey L C...
The Health Care Landscape Before
by phoebe-click
and After the ACA. Bill Evans. University of Notr...
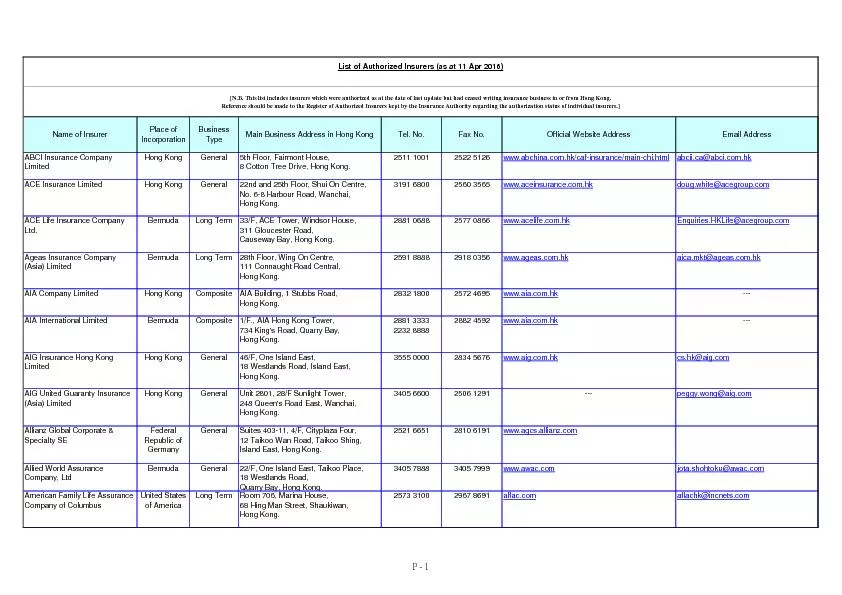
Name of InsurerPlace ofIncorporationBusinessTypeMain Business Address
by pasty-toler
www.abchina.com.hk/caf-insurance/main-chi.html ACE...
Solutions to address
by pamella-moone
poor data quality . DIA, Russian Federation. Ale...
require prior registration. Please contact the numberinformation.A fr
by susan2
Top Solutions VendorsServicesProducts Vendors' Ad...
DIRECTIONS TO NIHAFrom Baltimore Maryland
by ava
From I-495, take Exit 34 and stay in the far right...
US Department of Homeland Security Washington DC 20472
by miller
�� www.fema.gov W-16011...
COUNCIL OF GOVERNMENTS
by eleanor
SEDA-FEMA ELEVATION CERTIFICATE PROGRAMTOWN OF BLO...
INSURANCE INFORMATION
by harmony
PLEASE NOTE It is patient responsibility to coordi...
Patient Information
by nicole
Last Name First NameMiddle InitialSSN Home Ph ...
PATIENT INFORMATION HEALTH RECORD
by roberts
In order to help us render the proper podiatric se...
Letterhead of Agency or OCFS facility
by ella
Attachment Date To County Department ...
x0000x0000Revised 71013
by carny
REQUIRED CLINICAL INFORMATION TO PROCESS THIS REFE...
Financial Preparedness Training
by brianna
Facilitator Introductions. Facilitator Name. Facil...
Assignment of Benefits
by jovita
DOH - 4316 ( 10/11 ) N EW Y ORK S TATE D EPARTM...
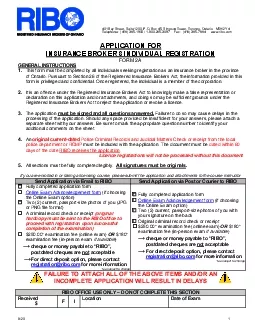
401 Bay Street Suite 1200 PO Box 45 Simpson Tower Toronto Ontario
by helene
8/201M5H 2Y4Telephone 416 365-1900 / 1-800-265-30...
Patient Information Confidential Patient Name Circle Male or Fema
by madeline
Insurance Information Name of Dental Insurance Co...
RINS Supplement 707
by valerie
CORPORATION or First and Last NameYour Social Secu...
I Date PATIENT REGISTRATION INFORMATION PLEASE PRINT D Mr O Mrs 0 Mi
by emmy
HEALTH HISTORY FORM FO GASTROENTEROLOGY ASSOCIATES...
Patient Access Management
by tatiana-dople
Leveraging Best Practices. Discussion Points. Bes...
Office of
by natalia-silvester
International Education. Swift Center, 1022 UTA B...
Local Government Pension Scheme Death grant expression of wish Your details Print clearly Full name Date of birth National Insurance number Address Postcode Employer Payroll number our expression of
by alexa-scheidler
I understand that x Hampshire County Council whic...
Patient Access Management
by faustina-dinatale
Leveraging Best Practices. Discussion Points. Bes...
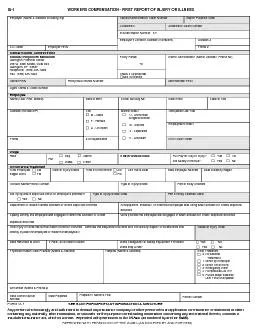
IA-1 WORKERS COMPENSATION - FIRST REPORT OF INJURY OF ILLNESS
by zoe
Employer (Name & Address Including Zip) Carrier/A...
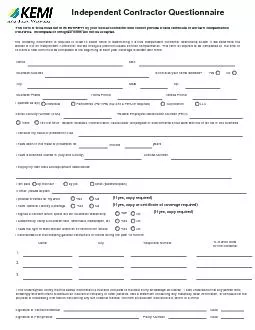
Independent Contractor Questionnaire
by alis
This form is to be filled out in its ENTIRETY by y...
What is the clinical question you would like the doctor to answer
by dandy
REQUIREDPatient146s possible neurological diagnosi...
Yorks First
by joyce
Bank Wall Street Fifth Avenue Street and Madison A...
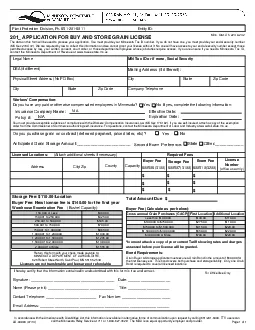
Storage Fee 11000LocationBuyer Fee New license fee is 14000 for the f
by erica
The data on this form will be used to process your...
VIDEOELECTRONYSTAGMOGRAPHY PATIENT INSTRUCTIONS
by molly
You have been referred to our office for an assess...
Applying to join the GCC
by cadie
The registrations team. Nick Jones. Chief Executiv...
Load More...