Explore
Featured
Recent
Articles
Topics
Login
Upload
Featured
Recent
Articles
Topics
Login
Upload
Search Results for 'applicant'
applicant published presentations and documents on DocSlides.
REQUEST FOR LIVE SCAN SERVICE Applicant Submission ORI A Type of Application Se
by sherrill-nordquist
O BOX 989002 Licensing Street No Street or PO Box ...
For validation only Private Security Guard License Application Send this completed form with a check or money order payable to the Department of Licensing to Public Protection Services Department of
by jane-oiler
Applicant information TYPE OR PRINT Name Last Fir...
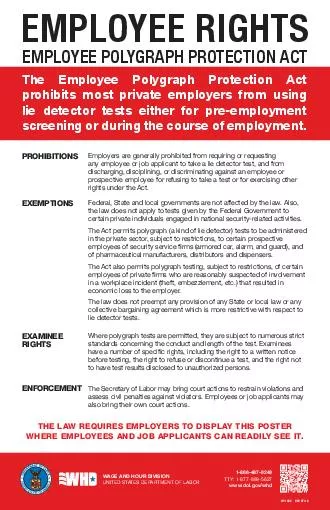
EMPLOYEE RIGHTS EMPLOYEE POLYGRAPH PROTECTION ACT PROHIBITIONS EXEMPTIONS EXAMINEE RIGHTS ENFORCEMENT Employers are generally prohibited from requiring or requesting any employee or job applicant to t
by marina-yarberry
Federal State and local governments are not affec...
ACC ACC CoverPlus Extra Application form Section Applicant details First name IR number Postal address Street City Postcode Suburb Email address Phone Area code Work number Code Other number Other
by karlyn-bohler
A partnership is the relationship existing betwee...
Section GOLD STAR FAMILY SELECT NEW PLATE BACKGROUND checked ABOVE AND SELECT NEW VANITY CONFIGURATION DATE SIGNED APPLICANT SIGNATURE Section VANITY PLATE REQUESTS CONFIGURATION Section MAIL PLATE
by debby-jeon
1014 DMV USE ONLY CC SPECIAL PLATE NUMBER DATE PR...
Prescription Advantag e Application Instruction Booklet Prescription Advantage Application Form for Massachusetts residents years of age and older or under age and disabled A
by calandra-battersby
Applicant and Spouse Information 573475734757347 ...
SECTION Applicant Information Patient should complete all information in Section
by calandra-battersby
Patients First Name US Resident Yes No Last Name ...
Granting Authority to Act Affirmation affirms the truth of the following Applicant Name
by kittie-lecroy
I am the of State relationship to business Name...
Declaration of Third Party Authorization to Act on Behalf of Applicant I Student Number Address hereby authorize the following person agent or agency to act on my behalf in all matters concerning my a
by olivia-moreira
I consent to the disclosure of all information co...
MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICES APPLICATION FOR GOOD CAUSE WAIVER Type or Print Clearly MO SECTION A APPLICANT INFORMATION LAST NAME FIRST NAME MIDDLE NAME PREVIOUS NAMES USED L
by luanne-stotts
Please fill out the Explanation of Background Scr...
Department of Alcoholic Beverage Control SUPPLEMENTAL DIAGRAM
by giovanna-bartolotta
APPLICANT NAME Last first middle 2 LICENSE TYPE 3...
GOVERNMENT OF INDIA MINISTRY OF HOME AFFAIR APPLICATION FROM FOR NON OFFICIAL TEMPORARY PASS Photo X cms Pasted and attested by gazetted officer Part I to be filled by the applicant Photo X cms Not t
by test
8 Residence Address and Telephone No 9 Mark of Id...
TD Form AnnexureI PROFORMA FOR APPLICATION FOR GRANT OF TIMBER DISTRI BUTION
by marina-yarberry
Name of Applicant 2 Occupation 3 Fathers Name...
APPLIC TION Valid through December HEAR NO Program age Dear Applicant Thank you for contacting the HEAR NOW Program of Starkey Hearing Foundation for hearing aid assistance
by tatyana-admore
Our hope is to provide hearing aids to those perm...
Page of MINISTRYDEPARTMENTOFFICE OF RGDWHG No Objection Certificate issuing officer should attest the photograph of the applicant with hisher signature and rubber stamp in such a way that half the si
by debby-jeon
NO OBJECTION CERTIFICAT 6KUL573626PW573620LVV5751...
State of Tennessee Department of Revenue Vehicle Services Division MediumSpeed Vehicle Affidavit Name of Applicant VIN As outlined in Tenn
by lindy-dunigan
Code Ann 551125 a vehicle may be registered as a...
PHYSICIANS CERTIFICATE FOR MINOR WORK PERMIT Name of Student Applicant in full Date of Birth Distinguishing Characteristics if any Sex Male Female PHYSICIANS APPROVAL School District Building Parent
by mitsue-stanley
Physicians Signature Date Signed IS NOT IS Limite...
FORM APPLICATIONCUMDECLARATION AS TO PHYSICAL FITNESS See Rule
by lois-ondreau
Name of the Applicant 2 SonWifeDaughter of ...
WORK SHARING PROGRAM Applicant Guide April Page Table of Contents A
by lindy-dunigan
Introduction B Eligibili ty Criteria
REQUEST FOR LIVE SCAN SERVICE Applicant Submission ORI CA Type of Application STATE GAMBLING LICENSE Code assigned by DOJ Job Title or Type of License Certification or Permit GAMBLING LIC CARD ROOM A
by karlyn-bohler
Street or PO Box Contact Na me Mandatory for all s...
AMERICAN BOARD OF COSMETIC SURGERY Certification Requirements Effective for the year The ABCS examination requires the applicant to be boarded by one of seven accredited boards listed below
by tatiana-dople
In addition s uccessful completion of an American...
Select one Limit requested VISA PLATINUM Number of cards requested VISA GOLD Number of cards requested VISA CLASSIC Number of cards requested VISA SECURED Number of cards requested APPLICANT
by lindy-dunigan
MEMBER EMANTSAL LAITINIELDDIM EMANTSRIF HOME ADD...
STATE OF FLORIDA SUBMIT THIS FORM TO YOUR LOCAL TAX C
by marina-yarberry
2 OWNER APPLICANT IDENTIFICATION BBBBBBBBBBBBBBB...
of INDIVIDUAL DETAILS DETAILS FOR JOINT APPLICANT TO BE GIVEN SEPARATELY MAILING ADDRESS FIRST INDIVIDUAL CITY TOWN DISTRICT PINCODE STATE COUNTRY PERMANENT ADDRESS IF DIFFERENT FROM ABOVE CITY TOW
by stefany-barnette
Account Opening Form for esident ndividuals 7KLV5...
art o be completed by applicant Name Please print or type Last First Middle Social Security number Candidates date of birth Address Number and Street City State ZIP School Ofcial Name CEEB Scho
by tatiana-dople
Under the Family Education Rights and Privacy Act...
APPLIC TION Valid through December HEAR NO Program age Dear Applicant Thank you for contacting the HEAR NOW Program of Starkey Hearing Foundation for hearing aid assistance
by natalia-silvester
Our hope is to provide hearing aids to those perm...
CPA LICENSING APPLICANT HANDBOOK CALIFORNIA BOARD OF ACCOUNTANCY INITIAL LICENSING UNIT Evergreen Street Suite Sacramento CA Telephone Facsimile Web www
by jane-oiler
cbacagov Revised 92 2014 brPage 2br CONTACT INFORM...
File IN THE MATTER between CHRIS TUCKER Applicant and JANET SMELLIE Respondent AND IN THE MATTER of the Residential Tenancies Act R
by marina-yarberry
SNWT 1988 Chapter R5 the Act AND IN THE MATTER of ...
Credit Card Payment Form Denotes Required Fields Applicant Name Name
by liane-varnes
brPage 1br Credit Card Payment Form Denotes Requi...
Allow Days for proce ssing or for the hearing impaired TD D Have you previously been issued a VA LIFETIME license No Yes Type Applicants Name Gender Male Female Please Print First M iddle In
by phoebe-click
00 NA NA NA NA Resident 44 and Under 26000 26000...
IDENTIFICATION APPLICANT STATEMENT Please state the requirements of the subcode from which a variation is sought
by mitsue-stanley
Use separate application forms for each variation...
APPLICANT Last Name First Name Middle Name Instruct ions to Reference On your organizations letterhead in English or Japanese please give your personal assessment of the applicants ability to partic
by karlyn-bohler
The most helpful reference letter will include 1 ...
CANADA SUMMER JOBS Creating Jobs Strengthening Communities Applicant Guide Table of Contents
by ellena-manuel
0 Purpose 20 Introduction 21 Objectives
Form see sub regulation of regulatio n Application Form for Grant of XVWRPVURNHUVLFHQFHXQGHUV ection of the Customs Act
by giovanna-bartolotta
Name of the applicant 2 Full address of the appl...
FORMAT OF APPLICATION FOR VERIFICATION OF TITLE
by mitsue-stanley
Name of the applicant in CAPITAL LETTERS 2 aName...
INDIAN COUNCIL FOR CULTURAL RELATIONS ICCR Scholarship slots under Africa Scholarship Scheme for the Academic Session Dear Applicant Thank you very much for your interest to pursue higher educati
by debby-jeon
As you prepare to apply for the Africa Scholarshi...
Ap plication Form nstructions to Applicant x Applicants must be at least years of age as of Friday th September x Make sure you have read the bout FACE In formation for Applicants prior to co mp
by karlyn-bohler
Attach additional pages if you require more space...
PTR icket Number Applicant Disputant Agent Officer I have consulted with disputant and determined their position and informed them of their right to appear and oppose the adjournment application
by lois-ondreau
A completed notification of adjournment applicati...
DEPARTMENT OF HEALTH AND HUMAN SERVICES Food and Drug Administration Silve r Spring MD NDA LABELING SUPPLEMENT AND PMR REQUIRED APPLICANT NAME ADDR ESS Attention CONTACT NAME TITLE Dear CONTACT Pl
by alexa-scheidler
Sections 505o3 and 505o4 and of the F ederal Food...
Applicant Please complete the following and sign Pursuant to the Family Education Rights and Privacy Act Buckley Amendment signed into law December I do do not waive my right of access to inspect
by test
pplicant57557s signature TO THE INDIVIDUAL PROVI...
Load More...