PPT-ANTIDIABETIC AND HYPOGLYCEMIC DRUGS
Author : narrativers | Published Date : 2020-06-15
Normal fasting range of blood glucose 60100 mg dL 3356 mmol L In general neurohormonal control of glucose production in healthy individuals maintains a
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "ANTIDIABETIC AND HYPOGLYCEMIC DRUGS" is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
ANTIDIABETIC AND HYPOGLYCEMIC DRUGS: Transcript
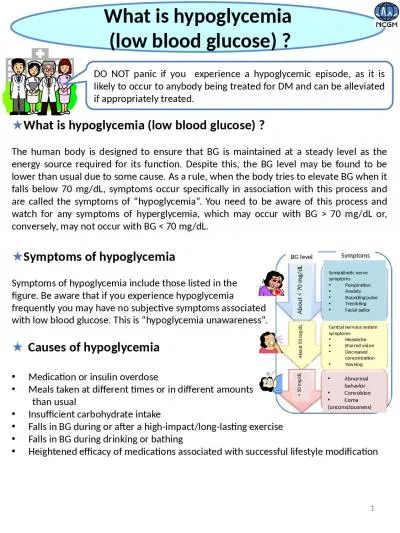
Normal fasting range of blood glucose 60100 mg dL 3356 mmol L In general neurohormonal control of glucose production in healthy individuals maintains a fasting serum glucose . LISTS 22 and 23 . 1. PHOBIA. Fear, dislike, aversion. Example: Someone who has a fear of feet is said to have “. podophobia. .” . 2. MIS. Hate (opposite of PHIL). Example: “The new leader has demonstrated that he is a misogynist.” (misogynist: a person who hates women). cvs pharmacy prescription discount card. It is now 2000, I am on permanent Social Security Disability. statistics prove prescription drugs are 16 400. pixiwoo best drugstore concealer. kansas statute possession of prescription drugs. Agonist Molecule Mimics . Drugs Prevent . Proper Reuptake. Drugs and Consciousness. Continued use of psychoactive drugs can lead to tolerance. Diminishing effect with regular use of the same drug requiring the user to take larger and larger doses before discontinuing the use of an addictive drug. OBJECTIVES. Name 5 . drugs. List and categorize each drug into their relevant drug class (A, B, C, Other. ). Identify the key effects of heroin, ecstasy and cannabis . Create a drugs awareness poster, implementing what has been learnt. Drugs and Consciousness. Continued use of psychoactive drugs can lead to tolerance. Diminishing effect with regular use of the same drug requiring the user to take larger and larger doses before discontinuing the use of an addictive drug. Powerpoint based on Holt’s . Lifetime Health. , 2009; chapters 9-10-11-12.. What’s Your Health IQ? . True/False. Side effects of over-the-counter medicines are rare.. Not following doctor’s orders while taking a prescription medicine can be dangerous.. :. http://learn.genetics.utah.edu/content/addiction/drugs/abuse.html. Drugs are either….. Agonists: . Mimic. . Reuptake inhibitors. Antagonist. s. : . Blocks. Reuptake . inhibitors. Drugs . terms:. Dermatologic Conditions. Diseases/Conditions Include:. Acne . Vulgaris. Acne . Rosacea. Psoriasis. Infections-. Bacterial. Fungal. Yeast. Viral. Dermatitis. Poison ivy. Diaper rash. Alopecia. Scabies. Although nausea and vomiting occur in a variety of conditions (for example, motion sickness, pregnancy, and hepatitis) and are always unpleasant for the patient.. The nausea and vomiting produced by . What are drugs?. A drug is considered to be any substance used either internally or externally as a medicine. . It can have an effect on the function or structure of living tissue through various chemical reactions. Diabetes Mellitus . Summary of Drugs Used in the Treatment of Diabetes. Diabetes Treatment . A person with . type 1 diabetes . must rely on . exogenous insulin . to . control hyperglycemia. , . avoid . Episodic sever Hypoglycemia . High level of insulin in hypoglycemic episode. High level of c-peptide . in hypoglycemic . episode. long periods without . hypoglycemia. relapse . after event-free periods of . evaluation guided by GC-MS analysis of ethyl acetate leaves extract of . Acacia . auriculiformis. . Benth. .. Naresh. Kumar . Rangra. 1,. *, . Subir. . Samanta. , . and . Kishanta. Kumar . Pradhan. The human body is designed to ensure that BG is maintained at a steady level as the energy source required for its function. Despite this, the BG level may be found to be lower than usual due to some cause. As a rule, when the body tries to elevate BG when it falls below 70 mg/.
Download Document
Here is the link to download the presentation.
"ANTIDIABETIC AND HYPOGLYCEMIC DRUGS"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents